Across The Room Assessment Triage

Triage In Emergency Department
Triage In Emergency Department
Nursereview Org Nursing Triage
Triage
Ppt Assessment And Triage Objectives Powerpoint Presentation Free Download Id 648526

Triage In Emergency Department Triage Waiting Room Team Leader Ppt Download
At anytime during triage if child determined to have an emergent condition triage should be stopped and treatment initiated nursing protocols may be initiated acuity level may change throughout the patient s stay in the emergency department re assessment when patient s in waiting room for 30minutes post triage level 1 red.
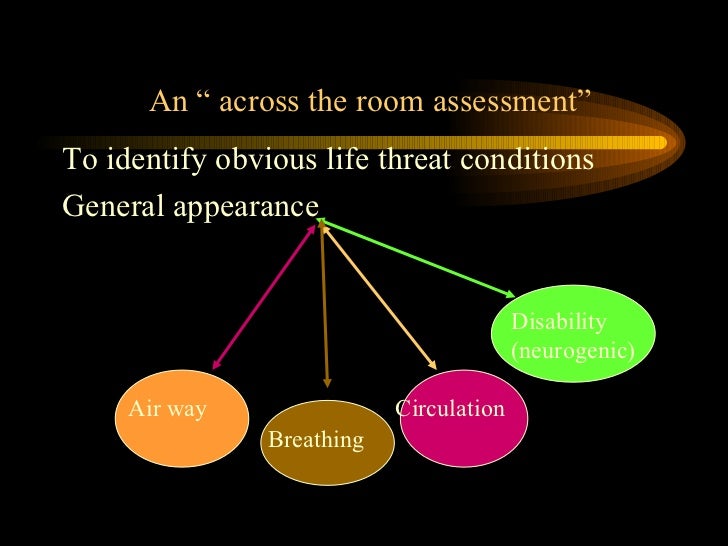
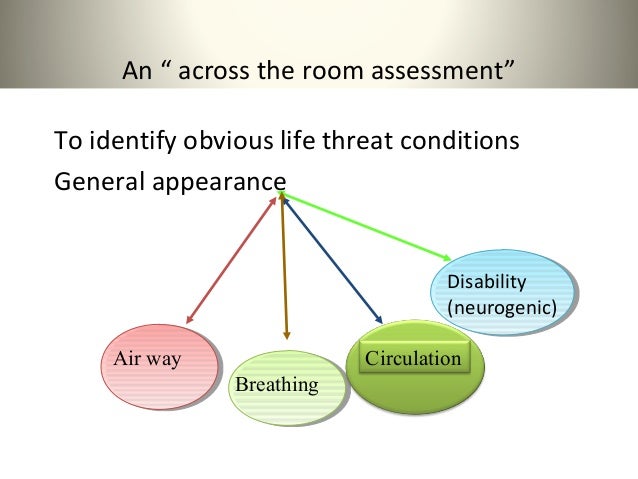
Across the room assessment triage.

Triage Nurse Key
Ppt Emergency Department Triage System Powerpoint Presentation Free Download Id 496899

Deputy Chairman Ed Ksmc Ppt Download

Triage
Pediatric Emergencies Ppt Video Online Download

Triage In Emergency Department Triage Waiting Room Team Leader Ppt Download
Gemc Trauma Triage For Nurses
Triage In Emergency Department Ppt Video Online Download
First Aid And Emergency Nursing Ppt Download

Triage In Emergency Department Emergency Department Human Diseases And Disorders

Free Er Triage Templates Invitation Templates Triage Nursing Nursing Assessment Emergency Room

Emergency Room Triage How Does It Work The Daily Scan
Triage And Transport Dr Suresh Babu Chaduvula

Cheat Sheet Rapid Assessment Emergency Department Nursing Flow Sheet Nursing Assessment Emergency Nursing Nursing School
Https Www Envisionphysicianservices Com Campaigns Breakthrough Series Presentation Materials Playbooks Ed Operations Management And Patient Flow Playbook Pdf

Is This Child Sick Usefulness Of The Pediatric Assessment Triangle In Emergency Settings
Https Neurolrespract Biomedcentral Com Track Pdf 10 1186 S42466 019 0036 Y

Pdf The Impact Of Senior Doctor Assessment At Triage On Emergency Department Performance Measures Systematic Review And Meta Analysis Of Comparative Studies
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcq4istaooylrpkklyixzs3hrjeywojz6rxenz7dvkcgq1ne3 1t Usqp Cau
Https Avera Cloud Cme Com Assets Avera Activity 12076 Esi 20in 20triage 20presentation Pdf

Reliability And Validity Of The Four Level Chinese Emergency Triage Scale In Mainland China A Multicenter Assessment Sciencedirect

Four Ways To Greatly Improve Emergency Department Triage

Development And Interrater Reliability Of The Uk Mental Health Triage Scale Sands 2016 International Journal Of Mental Health Nursing Wiley Online Library

How To Become A Triage Nurse Zippia

Emergency Department Quality Improvement Transforming The Delivery Of Care
Https Emcmedicaltraining Com Wp Content Uploads 2016 10 Tncc Prep Packet Revised June 2016 Pdf

Effectiveness Of Nurse Initiated Interventions On Patient Outcomes In The Emergency Department A Systematic Review Protocol Article Nursingcenter

Enpc Emergency Nurse Pediatric Class In Stockton Modesto Turlock Merced Ena Certified Emergency Nurse Association

Urgent Care Right Here Right Now Urgent Care Hospital Design Healthcare Design

What Is Triage Nursing

Triage Formal Emergency Department Triage Tools Are Inefficient Unfair And They Waste Time And Resources

The Greatest Good For The Greatest Number Triage In The Civil War And Today National Museum Of Civil War Medicine

Understanding The Triage Process In Our Emergency Department Upmc Western Maryland

Triage Tool For The Rationing Of Blood For Massively Bleeding Patients During A Severe National Blood Shortage Guidance From The National Blood Transfusion Committee Doughty British Journal Of Haematology

Coronavirus Disease Covid 19 A Primer For Emergency Physicians The American Journal Of Emergency Medicine
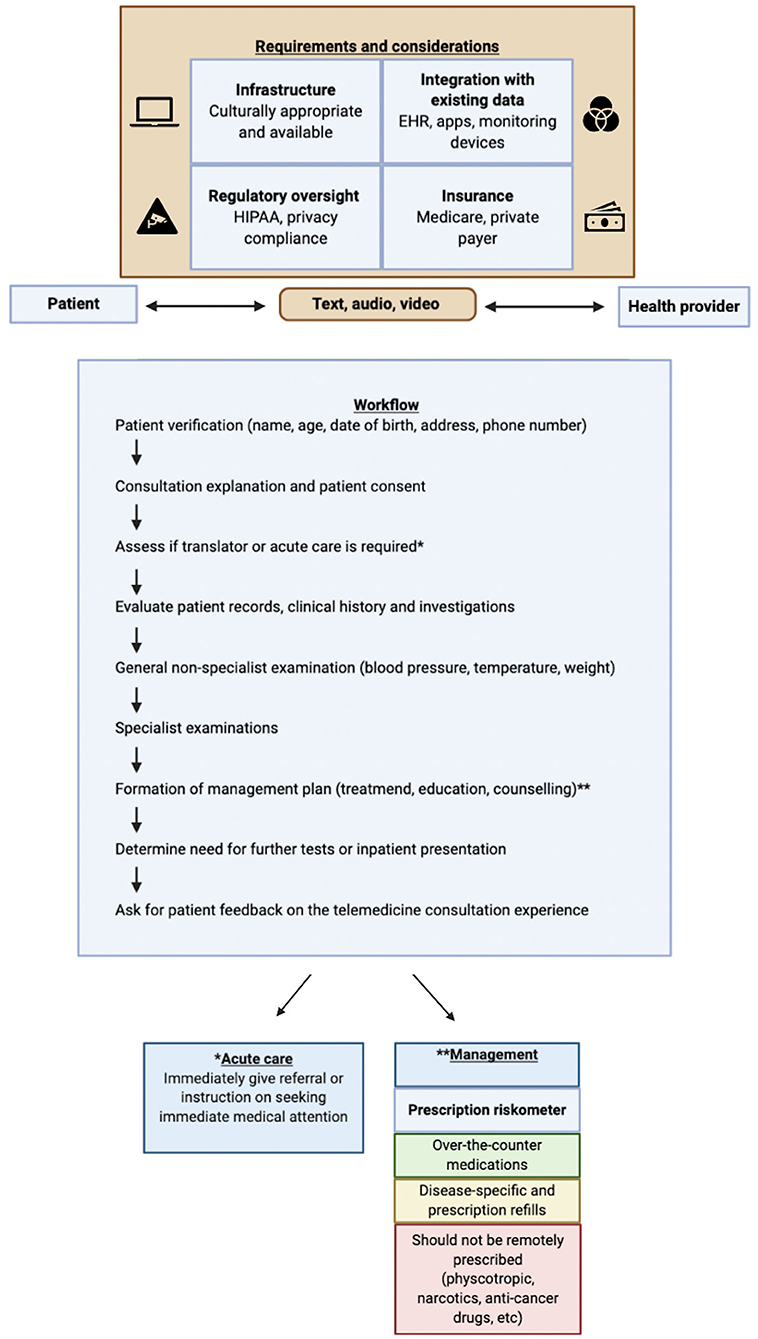
Frontiers Telemedicine As The New Outpatient Clinic Gone Digital Position Paper From The Pandemic Health System Resilience Program Reprogram International Consortium Part 2 Public Health

Pdf Emergency Department Triage An Ethical Analysis

Which Frailty Scale For Patients Admitted Via Emergency Department A Cohort Study Sciencedirect

Validation Of An Emergency Triage Scale For Obstetrics And Gynaecology A Prospective Study Veit Rubin 2017 Bjog An International Journal Of Obstetrics Amp Gynaecology Wiley Online Library

Patient Assessment Chart Emt Study Emergency Medical Responder Emt Paramedic

Obstetric And Fetal Triage Sciencedirect
Http Www Texaschildrens Org Sites Default Files Uploads Documents Health Professionals Kaleidoscope Day 202 20maternal 20fetal 20triage 20index 20tool Pdf

Nursing Resume Resume Examples Resume Writing Tips Nursing Resume Examples Rn Resume In 2020 Nursing Resume Examples Resume Examples Rn Resume
1
Source : pinterest.com
